|
ANNEX IV
INDONESIA COUNTRY REPORT
Ministry of Health, Ministry of National Education, Ministry of Social Affairs, Ministry of Public Works I. BACKGROUND The devastating effects resulting from the earthquake followed by the tsunami on 26 December, 2004 has tremendously stretched the capacity of the Nanggroe Aceh Darussalam (NAD) provincial government to provide social and health services along most of the western and northern coasts of Aceh. Enormous loss of life, massive destruction of homes, property and infrastructure have rendered people homeless and living in temporary often very crowded accommodation or with host families. Limited access to adequate basic services is also a contributory factor to the trauma suffered by survivors. This situation makes them vulnerable to the development of mental health disorders. In Aceh province the magnitude of the disaster is :( as of 31 March, 2005): · Death: 126.915 in Aceh Province and 128 in Nias (North Sumatra) · Missing 93.063 in Aceh and 25 in Nias ( North Sumatera) · Displaced population: Ø 514.150 in IDP camps in NAD Province Ø 260.000 in host families in NAD Province Ø 23.620 in North Sumatera ( 4000 Nias and 19.620 from NAD Province) Ø 1.615 in DKI Jakarta · Displaced population are distributed in Banda Aceh (49.921), East Aceh (13.709), Lhoksemauwe (24.494), North Aceh ( 27.112), Bireun (49,803), Pidie (85.860), Great Aceh (97.485), Aceh Jaya ( 40.422), West Aceh (72.689), Nagan Raya ( 17.040), South East Aceh ( 611), Sabang (3712), Central Aceh (5288), Simelue (18.009), South Aceh (16.148), South West Aceh ( 3480), Singkil (105), Aceh Tamiang (3224), Langsa ( 6156), Bener Meriah (648), Currently, there are 400,376 IDP’s in Aceh, approximately 250,000 IDP’s living with host family and 150,376 people in temporary tents or public building such as offices, school, mosques and barracks. Persons affected by a catastrophic event like a tsunami are exposed to extreme stressors not only immediately, but over a period of years. Many children have lost one or both parents. Many tens of thousands of families have lost one or more family members. There is substantial evidence that loss of livelihoods, particularly sudden loss, very frequently gives rise to severe anxiety and depressive disorders. These stressors could lead to serious mental health problems and disorders. Psychosocial and mental health provision should complement humanitarian work, starting in the first days and weeks of the relief effort, and should continue and be translated into substantial interventions through the rehabilitation and reconstruction phases. This is very important because too often there is a lack of awareness about the need for psychological and psychiatric support by health providers and the community, especially in the first few weeks of the aftermath. WHO estimates up to 50% of the affected population may be expected to experience significant psychological distress and 5 – 10% to develop a diagnosable stress-related psychiatric disorder. This means that approximately 1.2-2.0 million people will have considerable need for psychosocial support and up to 400,000 people may have trauma related stress disorders requiring skilled mental intervention. This additional burden to the existing mental health problems in the country will further strain the capacity of the mental and public health care givers in Aceh. This is compounded by the unavailability of some mental health personnel who may have perished in these disasters.
II. EXISTING PSYCHOSOCIAL SUPPORT ACTIVITIES In the immediate aftermath of the tsunami, related Ministries such as Education, Social Affairs and Public Works, with the support of international and national agencies and NGO’s started to provide psychosocial support to the survivors. However, in the early phase of the emergency, the situation was such widespread devastation that coordination among sectors was very weak. The collapse of the provincial government also created difficulties in service provision. Nevertheless, a lot of efforts were made to address the situation during the emergency phase. The following paragraphs describe the result of the interventions in the first three months. Health Sector The Ministry of Health started to address psychosocial support and mental health issues in day 3 after the tsunami. A call was made to mental health professional organizations to develop a draft for an immediate response. WHO also assisted the Ministry of Health in developing the MOH Action plan in mental health. The following activities were conducted as part of the implementation of the action plan: · A Rapid Assessment of Mental Health problems among survivors (5-10 January, 2005); · A set of technical guidelines were developed for providing psychosocial support for the general population and for children; · Mental health professionals were deployed to train: Ø Community leaders, religious leaders and women leaders to provide psychological first aid and psychosocial support. Three hundred and twenty people have been trained in Banda Aceh and Lhoksemauwe; Ø Primary health care workers in early detection and simple treatment of mental disorders and refer to specialized services, if necessary. Forty people have been trained in Banda Aceh and Lhoksemauwe; · Re-starting clinical activities in Banda Aceh Mental Hospital, including provision of psychotropic drugs; · Mapping of international and national agencies and NGO activities. There are many players providing psychosocial support in affected areas. However, efforts should be made to ensure that their interventions are evidence-based and sustained. As a first step, mapping of NGO’s activities in Aceh Province was conducted. It is expected that these activities will be updated from time to time; · Conducting coordination meetings among international and national agencies and NGOs as an attempt to prevent fragmentation, duplication and encourage standardization of mental health and psychosocial activities and programmes. These coordination meetings were conducted in Jakarta as well as in Banda Aceh and were supported by UNICEF and WHO. · Empowering the Provincial Health Office to monitor and supervise the programme (ongoing); · Establishing Satellite Health Posts in the new temporary shelters to provide health services for IDPs. The plan is to include psychosocial support and mental health as one of the services; · Printing posters and leaflets for distribution to temporary shelters and public facilities. These posters and leaflets provide information about symptoms of mental illness, where to go to for help and suggest simple coping mechanisms. Educational Sector Non Formal education · Establishment of 27 Community Learning Centers in Great Aceh, West Aceh , Banda Aceh and Nias CLC provides (a) Early childhood education (PADU), (b) Community Reading Center, (c) Equivalency Education, (d) Life skills trainings for income generation such as: automotive repair, sewing, cooking, acupressure, hair dressing, electrical installment, fishing, handicraft, etc. · Providing education materials to children · Collaborating with international agencies: Ø UNESCO and UNICEF provide training tutors; Ø USAID provide transportation to send education material; Ø National NGO’s (Sekolah Rakyat, Peace foundation, Syiahkuala University, etc) to provide tutors and other human resources. Social Sector § In the early phase of the emergency response, social support focused on logistics such as distribution especially of food, clothing, emergency tents and family kits. In addition, support was given for evacuation of survivors. This activity was conducted in collaboration with international and national NGOs such as UNICEF, Save the Children, Indonesian Red Cross (PMI), and Muhammadiyah. § Empowerment of the coastal communities. This was done through: ü Providing equipment for fishermen in collaboration with the Ministry of Ocean Affairs and Fishery; ü Establishing traditional markets for local merchants; ü Providing equipment, seeds and plants for local farmers. Infrastructures and Housing Sector Massive destruction of homes, property and infrastructure in urban and rural areas rendered people homeless and living in temporary tents, barracks and with host families. To begin to address this situation the following activities are conducted as part of the implementation of the action plan of the Ministry of Public Works: · Cleanning up garbages and debris, including corpse evacuation, particularly to open accessibilities (urban roads) and public service centers in Banda Aceh, Meulaboh and Calang; · Building of barracks (temporary shelters) for IDP’s relocation · 1,458 barracks have been built. Every barrack is designed for 12 families or 60 people, consists of 12 rooms, 1 public kitchen, 6 toilets and 1 water hydrant. · Building a multi-functional hall to facilitate different activities such as school, health center, etc for every 5 barracks; · Providing a clean water supply has been achieved by: Ø Improvement of temporary installation, water processing and distribution in Banda Aceh, Meulaboh, Nagan Raya; Ø Providing water supply for IDP’s through tanks, mobile trucks and public hydrants. · Improving temporary public infrastructure, such as road and bridge construction in Banda Aceh-Meulaboh, Medan-Tapaktuan-Meulaboh and Bireun-Takengon-Betong Ateuh-Meulaboh, to enable distribution of goods and assistance to survivors.
III. PROBLEMS ENCOUNTERED General Problems The tsunami was one of the greatest disasters that has occurred in the Indian Ocean region. Therefore it has attracted sympathy from all over the world. Despite this global effort, there are substantial problems that hinder optimization of the various relief efforts: 1. The total breakdown of the physical infrastructure. This condition inhibits a quick response. Transportation is severely damaged; the roads to the West Coast have only just been reopened at the end of March 2005. Many villages are not accessible by land, only by air using helicopters. The government is heavily indebted to the efforts of foreign assistance in providing this support, although indirectly, this problem provides additional mental health problem to the survivors. 2. Diminished capacity and quantity of human resources. Many of civil servants were lost, injured, dead, or lost their relatives. 3. Security is not totally assured. The long history of armed conflict in Aceh still poses an obstacle in reaching some affected sub-districts, even during the emergency relief phase. 4. Lack of confidence from the local community in governments’ management and the national emergency relief effort. This is as a result of the long-term internal conflict in Aceh, prior to the tsunami. 5. Language and cultural barriers. Most of Achene’s are conservative and religious values are heavily embedded in the local culture. The local language (Achene’s) is spoken for daily conversation. This situation should be taken into account sensitively in the recovery effort. Specific problems 1. Health Sector · Coverage of psychosocial support and mental health programmes is still limited due to limited human resources. In addition, movement of community leaders that had been trained creates difficulties in monitoring their performance. · Health workers and other civil servants also suffers from mental trauma that affects their performance. · Coordination among different levels of government is still weak. Not all decision makers put psychosocial support and mental health as a priority. · Capacity for the implementation of psychosocial and mental health programmes at province and district is relatively weak and needs strengthening. Part of it is due to the long neglected mental health programme in Aceh in particular and in Indonesia in general. · Health care providers are also overwhelmed by other competing programmes such as reproductive health, nutrition, child health, communicable disease, environment health and curative services. · Infrastructure development for service provision depends on other sectors. · There is no strong mechanism to supervise and provide consultation to PHC workers. 2. Educational Sector · Voluntary tutors are required, especially from the local community. · Temporary living conditions create difficulty for the process of education, teaching and learning. 3. Infrastructure and Housing Sector · Most of infrastructures were severely damaged, namely roads and bridge, water treatment, irrigation, telephone, electricity and ports. · In overall, 210 km roads and 110 bridges from Banda Aceh to Meulaboh are not functioning at all, because completely swept to the sea by tsunami while some others are now covered by sea water. · More than 100.000 houses totally damaged. · This severe damage to infrastructure result in a paralyzed economic activity. · Not all survivors are willing to stay in barracks that have been built. Many of them would like to go back to the previous homes, and start again with their previous work while maintaining ownership of their land.
IV. FUTURE PROGRAMME During the rehabilitation and reconstruction phases, the mental health and psychosocial programmes will need to consider the following elements in order to provide effective, evidence-based and culturally appropriate mental health service provision. 1. Health · Conduct periodic mental health assessments, to update the data related to psychosocial and psychiatric need and evaluate the interventions. · Strengthen the capacity of primary health care to enable early detection and simple treatment of mental disorders and to further refer to specialized services, if required. · Strengthen the capacity of the local community to provide psychological first aid and psychosocial support. · Establishment of community mental health teams. The Ministry of Health will provide 4 to 6 community mental health teams in selected district health offices. Ideal community mental health teams should consist of a psychiatrist, a psychiatric nurse, a social worker and a psychologist. The teams will support and supervise primary care services, conduct outreach and mobile clinical services for referred patients from the IDP camps, barracks and community. · Provision of mental health services for civil servant, soldier, police, volunteers in Provincial and District level. · Strengthening coordination meetings among international and national agencies and NGOs are required to prevent fragmentation and duplication and to standardize mental health and psychosocial programme activities. · Capacity building of Provincial and District Health Offices to develop programme, to collaborate with other sectors, to monitor and supervise the implementation of mental health and psychosocial programmes. 2. Education · To establish community learning center (CLC) in all relocation areas. · To provide mobile CLC for survivors who live with their families. · To provide extended life skill programmes. · To seek additional local tutors. · To provide training programme for local tutors. · To strengthen coordination among units in the Ministry of National Education. · To widen coordination among the concerned Ministries as well as with the local and international agencies and NGOs. 3. Infrastructure and Housing Public works infrastructures are to be constructed to support the realization of the selected spatial plan for the reconstruction of Aceh and Nias, in which the reconstruction of Infrastructure and housing includes : · Reconstruction of roads and bridges covers new construction of 210 km and major improvement of 526 km, among others : (i) Banda Aceh-Sigli-Lhokseumawe-border of North Sumatra, (ii) Urban roads in Banda Aceh, Krueng Raya & Meulaboh, and (iii) Banda Aceh-Lamno-Meulaboh. · Reconstruction of Settlements Infrastructures covers : (i) construction of water supply system including transmission and distribution pipes to cover 100 % urban and 50 % rural population, (ii) construction of sewerage system in Banda Aceh, Meulaboh, Lhokseumawe, and development of communal septictank compatible with with the existing system in 17 regencies/cities, (iii) construction of drainage system to cover 100 % urban and 10 % rural population, (iv) construction of urgent secondary, access and rural road to cover 100 % urban and 50 % rural population in 17 regencies/cities, and (v) development of solid waste & sanitary landfill to cover 100% urban population in 17 regencies/cities. · Construction of 66.500 new houses and improvement of 123.750 existing houses with standard type 36 m2 and can be developed to 45 m2. · Reconstruction of irrigation system 5.600 Ha and normalizing of 71 km river & 8 km seashore.
V. CONCLUSION · Because of its geographic location Indonesia is particularly prone to natural disasters. In addition, the risk of man made disaster is also increasing. This condition puts the Indonesian population to high risk of exposure to extreme stressors that might result in psychosocial problems. · All efforts which have been undertaken by national, local government and the international community is still not yet adequate. Therefore, we are in need of long-term aid which does not only relate to the tsunami, but to equip the country to deal with disasters in general. It is important to assist the Indonesian government to become prepared in face of another disaster. · International assistance and support has been outpouring to the affected area for immediate emergency relief as well as for the rehabilitation and reconstruction process that requires a longer period of time. However, frequently the focus of rehabilitation and reconstruction phase is on building infrastructure. Therefore there should be a commitment to allocate sufficient resources for rehabilitation of the people, including development of sustained psychosocial support and mental health programmes. · Mental health professionals should work in close partnership with experts from other disciplines to ensure that relevant social interventions are fully implemented. INDIA COUNTRY REPORT
Medical Relief in Tsunami affected Areas in India
Emergency Medical Relief Division Directorate General Of Health Services Ministry Of Health And Family Welfare Government Of India
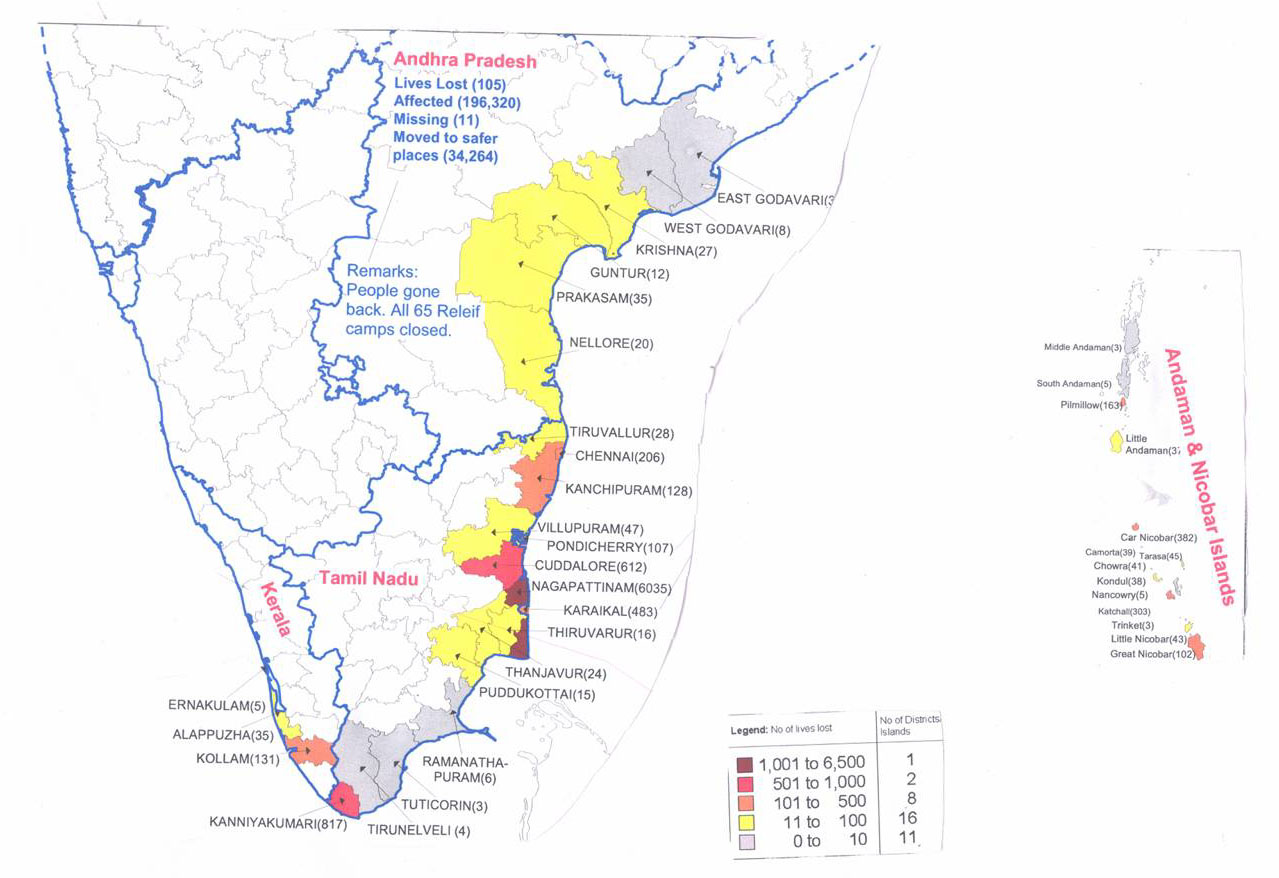
Tsunami Impact – States Affected
Damages due to Tsunami – A& N Islands
Damage due to Tsunami – Tamil Nadu
Damage due to Tsunami – Pondicherry
Damages due to Tsunami – Kerala
Damage due to Tsunami – Andhra Pradesh
Total Damage due to Tsunami
Rescue and Relief
Prime Minister’s Visit To Affected Areas
Response by the Ministry of Health and Family Welfare
Public Health Response
Public Health Response
Central Medical Teams to A&N Islands
Emergency Medical Relief
Emergency Medical Relief
Wayside Clinic
Emergency Medical Relief
Emergency Medical Relief
Psychosocial Support
Psycho-Social Care
Strengthening of disease surveillance
Strengthening Of Disease Surveillance
I.E.C Health education activity intensified by health education teams in various Tsunami affected islands. Health Education in a Relief Camp
Nutritional Surveillance The National institution of nutrition under ICMR and nutrition Dep't of All India institute of hygiene and Public health is co-coordinating to undertake nutritional surveillance in the relief camps of Port Blair and the remote islands of Little Andaman, Car Nicobar, Camorta (Nancowry Group), Katchal ( Nan Cowry Group), Little Nicobar, and Cambell Bay. Assistance to other countries affected by Tsunami - Sri Lanka-I
SRI LANKA –II
Aid to Maldives
Aid to Indonesia
Post Tsunami Psycho-Social Care Emergency Medical Relief Division and National Institute of Mental Health and Neuro Sciences, Bangalore Government of India • National Institute of Mental Health and Neuro Sciences, Bangalore [NIMHANS] identified as the Nodal Agency. • Need assessment carried out. • All major Mental Health Institutions involved. • Immediately over 100 mental health professionals mobilised from Government sector. • Affected area divided into six zones. Zonal in-charges identified. • Teams constituted having Psychiatrists, Psychologists, Social Workers and Psychiatric Nurses. • Local area needs such as language kept in mind while constituting the teams. • The teams adopted Camp Approach. Set up Mental Health clinics in large camps. • Provided OPD Services • Indoor services provided by the nearest mental health facility. • Camp units held sensitisation sessions for the camp volunteers and health workers. • 60-80% of the affected population exhibited one or the other symptoms related to Post Trumatic Stress Syndrome • The most common symptoms were: Excessive Grief, Troubles with repeated Flash back; sleep disorders; excessive fear; continuing in a state of shock; alcohol abuse; exaggeration of existing illness; Death wish & suicidal ideation. • Vulnerability Assessment done • Population prioritized on the basis of: – Those with multiple deaths in the family – Those who have lost the spouse – Those who have lost child/ Children who have lost parents – Those with previous mental disorder. – Those who have lost home. • 2250 patients with severe psychological symptoms were treated. • 3500 patients counseled individually • 35,000 counseled through group counseling. • Activities still continuing in affected areas. Critical Needs • Massive capacity building efforts • Evidence based interventions • Co-ordination/Net working Capacity Building • Seven training hubs activated • Six day training for TOTs held • 110 three day training workshops held for Health proffessionals and health workers. • 4387 trainers trained in two months. Future Plan of Action • Strengthen/ implement District Mental Health Programme in worst affetced districts. • Enhance availability of trained personnel through: • Six day TOT programme on fortnightly basis. • Co-ordinate and organize three day training programme in as many affected areas as possible. • Networking for undertaking for the training programme. • Sensitisation workshops for district level administrators. • TOT Training for NGOs , local self Government functionaries, school teachers, anganwadi workers. • Monitoring of the ongoing activities • Co-ordination with NGOs/ International agencies. • Develop strategy for district level micro-planning • Regular Review meeting for sustainability MALAYSIA COUNTRY REPORT
Department of Social Welfare (DSW) Malaysia The purpose of this report is to provide information on the Tsunami Disaster which struck Malaysia on 26 December, 2004 and actions taken by the Malaysian Government to provide relief aid to the victims. Introduction
- District Natural Disaster Relief Committee - State Natural Disaster Relief Committee - National Natural Disaster Relief Committee Structure and Mechanism In practice DSW being a member of the National Disaster Management and Relief Committee plays its roles before, during and after the occurrence of the disasters and is responsible in giving help and to rehabilitating the victims. Its four main functions and responsibilities are;
Short Term Scheme
The DSW Malaysia is responsible for the acquiring, storing and distribution of food before, during and after the occurrence of disaster. The DSW also decides on the quantum of daily rationing of food supplies to the victims. Long Term Scheme
THE TSUNAMI The incident that occurred on 26.12.2004 affected the coastal areas of five states in Malaysia. 1. Perlis. 2. Kedah. 3. Penang. 4. Perak. 5. Selangor. The disaster resulted in the loss of 68 lives and 2848 families (7827 persons) were forced to evacuate their homes and were placed in evacuation Centres. Estimated los incurred was RM18.7 millions. Immediate Action Taken by DSW
The Evacuation Centres
Provision of Financial Relief
As of 3 January 2005, a total of RM2,270,600.00 were dispersed to victims affected by the disaster. This amount does not include the cost of operation of the 33 evacuation centres throughout the affected states.
Counseling Services · Counseling services were immediately rendered to the victims at the evacuation centres in order to minimise the effects of the trauma experienced (post trauma counseling) . · Action taken are; a) Registration of victims b) Psychological Support c) Assessment reports d) Walk in counseling at the centres e) Visits to the houses of victims. · These were undertaken by registered counselors from DSW, and also volunteers from NGO’s and also local universities. Other Activities
Present Status of Operational Transition House
· The transition houses were build within one month after the incident. · The Malaysian Government is also collaborating with the corporate sector to rebuild houses for those badly affected. · The State Governments have also allocated land for rebuilding houses and for resettlement. · Victims who are still staying and receiving help at the evacuation centres are those who have experienced total loss of their belongings including houses. · The rest are back to their homes and have resumed their daily activities. Those with minor or partially destroyed houses were given financial aid to do repairs with the help of NGO volunteers. Conclusion
District of Langkawi, Kedah
Proposed resettlement site under construction District of Langkawi, Kedah
Work in progress including a playground District of Langkawi, Kedah
Completed house and inside view District of Kota Kuala Muda (Kedah)
Proposed site for resettlement and rows of transition home District of Kota Kuala Muda (Kedah)
Child Activity Centre and an inside view. Tanjung Bungah, Penang
Transition houses for 39 families Tanjung Bungah, Penang
Child Activity Centre Tanjung Bungah, Penang
New site for resettlement SRI LANKA COUNTRY REPORT
Post Tsunami Psychosocial work – a local experience from Sri Lanka M. Ganesan 4. 4. 2005
Pre tsunami Situation • Very few psychiatrists 4 in the tsunami affected areas • Mostly general hospital inpatient care 4 inpatient units • Hardly any community care few outreach clinics and some community follow up The National Picture (-) • High, unrealistic expectations • Little understanding of the local situation • Very little assessment of local capacity • Confusion and conflicts between stake holders • Inability to define the field • Inability of the ministry to meet the manpower needs of the most affected areas The National Picture (+) • Interest shown at the highest level President, minister • Ministry of Health identified as being responsible for Psychosocial work • High priority at ministry level gave the opportunity to mobilize the PHC system • Some guidelines and training schedules The Solution Each region (service providers) selected the model and strategy which they felt would be most suitable to their regions.
The Effect of Tsunami in Batticaloa Tsunami affected over 250,000 people directly, with nearly 70,000 persons currently displaced (approx. 38,000 in welfare camps), 2,846 confirmed dead, 1,027 missing and 2,375 injured The Batticaloa Approach • Psychosocial in the broadest sense • Definition “psychosocial” refers to the dynamic relationship that exists between psychological and social effects, each continually inter-acting with and influencing the other. • Coordination and improving capacity The Strengths • Good local network NGO + Government • Local governmental support good Health Education Police • Experience in war related work The Mangrove • The Psychosocial coordinating body • Around 40 members • Included both Governmental, UN, NGO The Mangrove Objectives 1 To facilitate technical support to all organisations involved in psychosocial response to the tsunami disaster, to enhance the quality of services provided to affected persons. The Mangrove Objectives 2 To coordinate and synchronise the various efforts by state, non-government and other groups to provide psychosocial interventions for persons affected by the tsunami disaster. The Mangrove Objectives 3 To liaise with the state institutions and other agencies involved in relief, resettlement and reconstruction work to promote practices that enhance or protect the psychosocial wellbeing of affected populations. The Mangrove Core Values 1 • Non controlling • Supporting • Focus on tangible outputs; solution-focussed rather than problem-focussed • Commitment to low running costs • Responsive to external needs and opportunities • Inclusiveness • Respect for diversity in a) theoretical approaches b) gender / ethnicity / religion / c) local cultural practices and approaches, modes of healing The Mangrove Core Values 2 • Emphasis on enabling and engaging members rather than regulating them • Critical • Practical • Commitment to a long-term perspective • Respect for interests of local groups • Place priorities and perspectives of survivors at centre of psychosocial services • Focus on best practices - informed by prior experiences Activities of the Mangrove • Mapping of district services, activities and actors at a district and DS division-level • Training programs – tsunami awareness etc • Burnout prevention –arrange supervision • Good practice guidelines- play activity • Linking up organizations – identification tent • Setting and implementing minimum standards – gate keeping • Assessment of services at community level Activities of the Mangrove • Constituting a Resource Group (drawn from local and external personnel) • Facilitation and design of progs / activities – emergency plans for schools • Counselling and therapeutic services • Training of workers and community groups • Mediation in turf problems • Interacting with national-level processes related to policy-formulation and programming within the state and non-government sectors Activities of the Mangrove Lobbying and provision of input from a psychosocial perspective into key relief, resettlement and reconstruction structures / focal points for the district. - Through the task force The Advocacy • One of the 8 task forces (protection and psychosocial) • The Task force Chair - Psychiatrist Co Chair - UNHCR • Members of the task force The Mangrove Women coalition/ GBV Task force Child protection committee Meet other task forces once a week Service provision at local level • 6 DS divisions affected • To have a referral and assessment points at this level • Will have both health and NGO staff • Will work closely with field level workers • Will have a second level staff to refer to Problems • Little awareness among public on psychological help and services • Competition between organizations • New organizations coming in with very little study or consultation – Malaysia team • Pressure from funding agencies on local organizations to expand • Some reluctance to share knowledge and skills • Input into coordination mechanism by the organizations poor Activities by partners of The Mangrove • Befriending • Play • Counseling • More intensive/ medical therapy Referral system (planned)
THAILAND COUNTRY REPORT Post-Tsunami Mental Health Assessment Department of Mental Health, Thailand Ministry of Public Health Thailand MOPH – U.S. CDC Collaboration Centers for Disease Control and Prevention Briefing at the DoMH March 08, 2005
Objectives Among tsunami-affected populations and relief workers in Phang Nga, Phuket and Krabi: 1. Assess the prevalence of post-disaster traumatic stress, disaster related psychiatric impairments, psychological co-morbidities and associated factors 2. Identify mental health needs and areas for post-disaster mental health interventions and support 3. Assess whether increased mental health interventions and support efforts have been successful in lowering negative post-disaster mental health effects
• Populations • Displaced persons • Persons in the community • Children ≥ 7 – 14 years • Relief workers • Location • Phang Nga, Krabi and Phuket provinces • Time • February 14 - 22, 2005 • 8 weeks post-disaster
• Methodology – Representative samples of displaced persons, community and children • Multi-stage cluster sample with proportional to size representation – Simple random sampling of households according to camp size (Phang Nga) – High and low impact areas – 3 affected and 3 non-affected sub-districts – 8 villages each – Simple random sampling of households according to village size – Convenience sample of relief workers • Sample size calculation – Assumptions • Camps 15% PTSD: n=392 (95% CI +/- 5%) • Community 12.5% PTSD: n=323 • Children 12.5% PTSD: n=163 • Relief workers 10% Mental Health Problems: n=138 • Instruments – Demographics, general health – Harvard Trauma Questionnaire for post traumatic stress disorder (PTSD) – Hopkins Symptoms Checklist (anxiety, depression and distress) – UCLA Child PTSD – Berleson Child Depression Scale • Data collection methods – Palm-pilot interviewer administered questionnaire • 33 trained interviewers from Bangkok, Surat Thani and Song Khla • 5 IT staff • Daily download of interviews using Hotsync and electronic transport to Bangkok using GPRS Training and IT Preparation, Phuket, February 14, 2005
Data Collection, February 15-22, 2005
Post-Tsunami Mental Health Assessment – Adults
Post-Tsunami Mental Health Assessment - Children
• Relief workers – Very high percentage exposure to human remains, people dying etc – Very few mental health problems – Needs to be looked at more in detail Conclusions • Unique collaboration has led to a successful and solid study, providing valuable information for back-up and guidance of mental health interventions • Representative sample of displaced persons, children and the community • High percentages of mental health problems – PTSD lower than elsewhere, both in children and adults – High trauma exposure levels in children – Distinct differences between camps, community and high and low impact areas – Very low levels of mental health problems in relief workers, despite high exposure • Data need to be analyzed further
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||